

 Disha Shetty
Disha Shetty
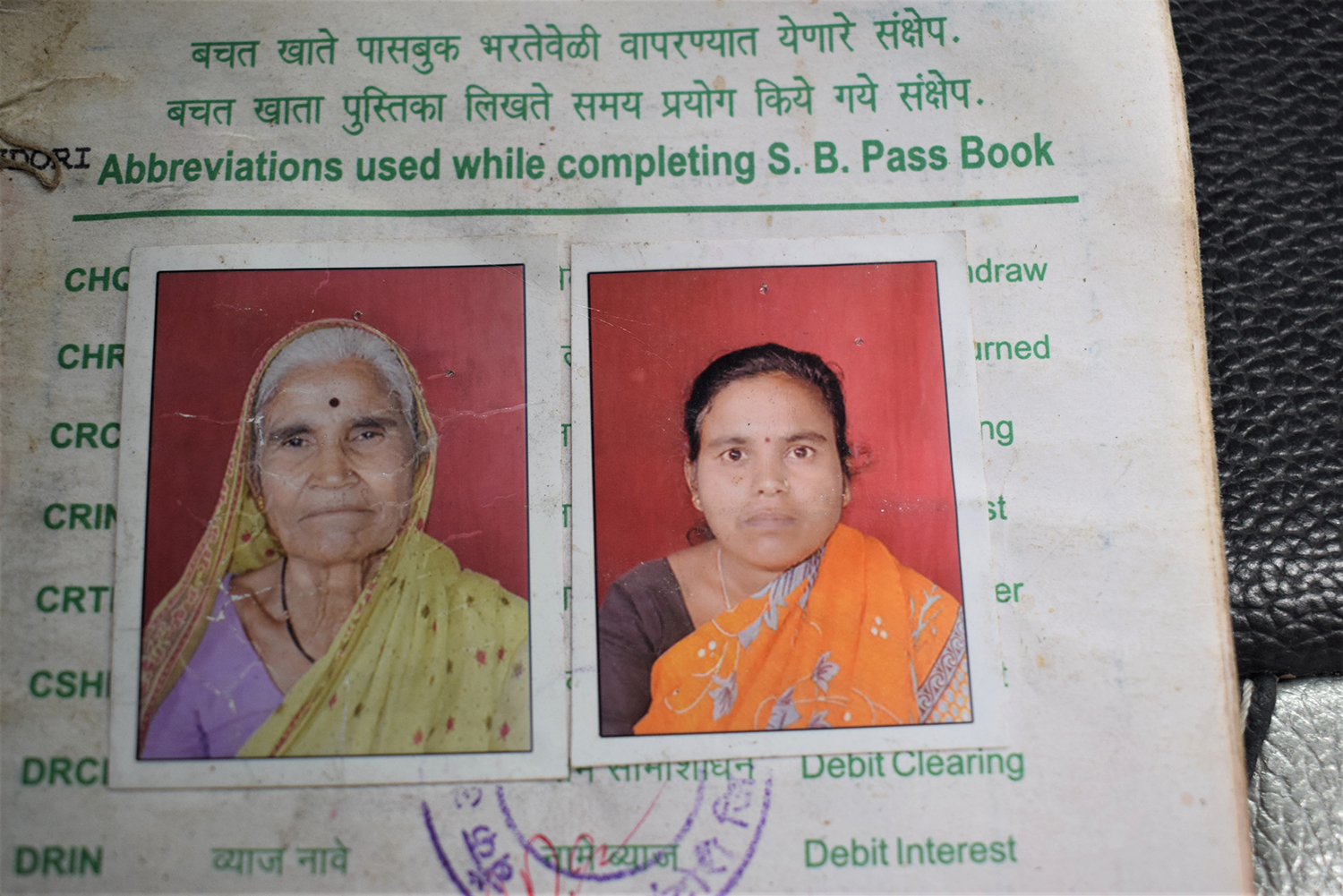
Mysterious deaths of mother, daughter lay bare neglect of rural healthcare in India
The deaths of a village elder and her daughter during India’s second COVID-19 wave raise important questions about lapses in the Indian government’s pandemic response.


