


Women are twice as likely as men to die from heart attacks.
When a nonsmoker dies of lung cancer, it’s twice as likely to be a woman as a man.
And women suffer more than men from Alzheimer’s and autoimmune disease.
Yet research into these conditions, and many more, generally fails to examine women separately. It’s even less likely to look at disparities affecting women of color — why, for instance, Black women are nearly three times more likely to die in pregnancy than white women are.
It’s been 30 years since Congress ordered the National Institutes of Health to make sure women were included equally in clinical trials. But despite some progress, research on women still lags, and there’s growing evidence that women and girls are paying the price.
“Research on women’s health has been underfunded for decades, and many conditions that mostly or only affect women, or affect women differently, have received little to no attention,” first lady Jill Biden said in announcing a new White House Initiative on Women’s Health Research on Nov. 13.
“Because of these gaps, we know far too little about how to manage and treat conditions like endometriosis, and autoimmune diseases like rheumatoid arthritis. These gaps are even greater for communities that have historically been excluded from research — including women of color and women with disabilities.”
Not only do researchers fail to include enough women in clinical trials, they often don’t look for differences between how men and women respond to treatments.
The new initiative acknowledges that Congress’s earlier directive fell short.
“What most people don’t recognize is that it was advisory. It was a recommendation,” said Dr. Nanette Wenger, a top cardiologist in Atlanta whose work helped propel the NIH legislation. Wenger says the 1993 law that she spent so much time pushing failed to reach its goals: “It had no teeth.”
The new White House initiative doesn’t have many teeth yet, either. It directs the U.S. Departments of Health and Human Services, Defense and Veterans Affairs, as well as several major White House offices to recommend “concrete actions” the Biden Administration can take within 45 days.
Over the years, officials at the NIH have urged researchers to include more women in the clinical trials that study disease and potential treatments. But the drug development process is long and complex. Efforts to increase diversity of all kinds in medical research run up against overburdened investigators, overwhelmed physicians and a U.S. Food and Drug Administration pulled between a demanding public clamoring for new drugs and a pharmaceutical industry driven by profits. So questions about gender differences fall through the cracks — and the lack of research means no one can even hazard a guess as to all the consequences.
“We know less about female biology and we are struggling to catch up,” said Dr. Janine Clayton, director of the NIH’s Office of Research on Women’s Health.
On the surface, things look good. More than half of the people in NIH-funded clinical trials are female — 58.5%. And more medical trials focus only on women than only on men.
But it takes only a light scratch to see the numbers are misleading.
Pregnant and nursing women are still greatly underrepresented in clinical trials. So are Black, Hispanic, Asian and Indigenous women. Women make up more than half the U.S. population, but account for just 43% of volunteers in cancer trials, 46% of those in immunology trials and 42% in kidney disease trials.
Even trials involving the latest weight-loss drugs — which enrolled more women than men — have failed to determine whether women respond differently to the hormone-based treatments.
It’s a legacy stemming from decades in which women were blocked from clinical trials, in part because of concerns related to pregnancy and menstrual cycles and in part because researchers bought into the now-debunked idea that women were working and taking care of families, and therefore too busy to participate.
As a result, women are still less likely to be included in trials for treatments for the biggest killer of both men and women: heart disease. Even lab mice are predominantly male, and cell lines used in the early stages of medical studies come primarily from men.

The effects show up in almost every aspect of human health.
While women are about as likely as men to have heart attacks, they are more likely to die from them, according to the NIH’s Office of Research on Women’s Health.
Women are more likely than men to suffer from autoimmune diseases such as rheumatoid arthritis, but the reasons are poorly understood. And even though women suffer more from chronic pain than men do, they are less frequently treated for it.
The U.S. has by far the worst maternal mortality rate of any comparable country and is the only developed nation where those numbers are climbing.
These deaths cannot all be prevented by better research. But the lack of attention to how women respond differently to drugs, how medical providers treat women and how the system still provides women less-than-adequate care is costing lives, experts and advocates say.
“Because of research, we know that sex matters,” Clayton said. “We’ve made a lot of headway since considering women too fragile or might become pregnant as a reason for exclusion,” she added. “Because of research we know that even down to the cellular level, the genetic level, there are sex differences in those cells.”
Nonetheless, many researchers overlook those differences.
“We still have the same problem that we had 30 years ago,” said Dr. Stephanie Faubion, medical director of The Menopause Society and director of the Mayo Clinic Center for Women’s Health in Jacksonville, Florida. “We still don’t know if these drugs work the same, better or worse in women than in men.”
A series of studies called the STEP trials, published in 2021 and 2022, are the latest example.
They have shown that the diabetes drug, semaglutide, sold under the brand names Wegovy, Ozempic and Rybelsus, can help obese people lose up to 15% or more of body weight in just over a year and can treat heart disease. The resulting clamor for the drug has caused shortages.
Faubion was researching whether the drugs have different effects among women taking certain medications for breast cancer. “We think estrogen has something to do with the weight loss,” she said. But none of the trials — published in prestigious medical journals such as the New England Journal of Medicine and the Journal of the American Medical Association — break out separate data on men and women. “We can’t do it if we can’t get the data. It’s stunning,” Faubion said.
Some efforts have been made to address the problem. The NIH and FDA have offices dedicated to ensuring equity not only for women, but for ethnic and racial minorities as well. However, neither agency fully enforces its regulations and policies on sex differences in research, advocates said. “All you have to say is, ‘Oh, yes. We considered it,’” said Katie Schubert, president and CEO of the nonprofit Society for Women’s Health Research. “You don’t have to actually do anything about it.”
Researchers are rarely forced to use a gender lens to interpret their findings.
“There’s no mandate to analyze the sexes in different ways,” said Dr. Nicole LeBoeuf, an associate professor of dermatology and cancer specialist at Brigham and Women’s Hospital in Boston. Without analysis, investigators cannot tell if there are sex differences to consider in diagnosis or treatment.
Fewer than a third of the results from the most advanced clinical trials, known as Phase III trials, are reported by sex in medical journals, Clayton said. Doctors rely on the journals to inform their practices. If there’s no data to justify changing how they treat women, they don’t.
Perhaps as a result, emergency room staff take longer to treat women who complain of heart attack symptoms. And doctors and patients alike often miss stroke symptoms among women, even though they have a higher risk than men.
Lung cancer, the biggest cancer killer by far, mostly affects smokers. But every year, it kills 20,000 to 40,000 nonsmokers in the U.S., according to the Centers for Disease Control and Prevention. Two-thirds of them are women, said Dr. Claudia Henschke, a lung cancer expert at New York’s Mt. Sinai Hospital. Still, just a tiny fraction of research on lung cancer focuses on women.
The FDA, which must approve drugs before they reach the market, is clear: Including more women and people of color in clinical trials is desirable, but only for the sake of having a representative sampling of the population, not to focus attention on those groups. Senior FDA officials say a one-size-fits-all approach is the most realistic way to test drugs for everyone.
Evidence shows that doesn’t always work.
‘Where are the data about treating women?’
By the late 1980s, Wenger realized she was missing critical information. As a senior cardiologist at Atlanta’s Grady Memorial Hospital, she noticed a disturbing and counterintuitive pattern. It wasn’t only men who were dropping dead of heart attacks.
“When I began to look and ask, ‘where are the data about treating women with heart disease,’ there were none,” said Wenger, who continues to practice at Grady and teach at the affiliated Emory University medical school.
She asked the American Heart Association and the NIH for studies to guide her. “People sort of shrugged their shoulders and said, ‘Well, there’s no difference. And it doesn’t matter,’” she said.
Given the toll of heart disease on both women and men, Wenger was flummoxed by the lack of interest.
Wenger persuaded the NIH to sponsor research that resulted in a startling article in the New England Journal of Medicine in 1993. It showed disparities by gender across the spectrum of heart disease, from heart attacks to strokes, high blood pressure and heart failure. Not only was more research needed, the article concluded, but a change in attitude among doctors was vital.
The findings helped accelerate a movement that led to passage of the bipartisan 1993 NIH Revitalization Act directing the agency, which funds most medical research in the U.S., to ensure that women and minorities were included and to establish guidelines for doing so. The FDA set similar guidelines the same year.
In 2016, Congress got more specific, requiring scientists conducting Phase III trials to not only include data on sex, gender, race and ethnicity, but to analyze it.
But gender disparities in medical research persist. “NIH applies a disproportionate share of its resources to diseases that affect primarily men, at the expense of those that affect primarily women,” a 2021 report in the Journal of Women’s Health concluded.
“It’s sad that what we have done feels like a drop in the bucket,” said LeBoeuf.
Only 4.5% of the money spent researching coronary artery disease goes to projects that focus on women, according to a 2022 report by the advocacy group Women’s Health Access Matters (WHAM), written with the Rand Corporation. While women are disproportionately affected by rheumatoid arthritis, a mere 7% of research into the autoimmune causes of the disease looks specifically at women. Likewise, only 12% of Alzheimer’s research and 15% of lung cancer research centers on women.
Widespread caution
Some of the biggest drug disasters in history have affected pregnant women and their babies. Thalidomide, prescribed widely in the 1950s to treat nausea in pregnancy, caused severe birth defects. Diethylstilbestrol (DES), a synthetic hormone prescribed to pregnant women between 1940 and 1971 to prevent miscarriage, premature labor and other complications, was later found to raise the risk of cancer in children, especially girls, exposed in the womb.
Those medical failures prompted widespread caution about enrolling women who might become pregnant during clinical trials. Although the FDA lifted this restriction in 1977, pregnant and nursing women remain greatly underrepresented in medical research. “If a woman becomes pregnant during a clinical trial, it is considered an adverse effect and the woman is taken off,” said LeBoeuf.
That leaves millions of pregnant women without tested options to treat serious diseases. “No pharmacological treatments for sickle cell disease have been studied in pregnant people,” Dr. Lydia Pecker of Johns Hopkins Medicine said at a recent NIH workshop.
Physicians and advocates say it’s difficult to change decades of practice.
Even FDA believes there’s no problem
The argument that sex differences are rarely significant persists, even at the top levels of biomedical research.
“FDA always looks at results by sex,” said Dr. Janet Woodcock, the agency’s principal deputy commissioner. “Usually there are not differences, but there are important exceptions where differences matter. If significant trends are seen by sex, we look into it and may note it on the drug label.”
But science isn’t the only consideration; economics are also in play. Pharmaceutical companies want to get drugs approved as quickly as possible. “They are going to do the minimum it takes to get on the market,” Woodcock said. “Companies try very hard to dose everybody at the same dose. It is very unpopular to put out a drug and say, ‘these folks need a different dose.’ Clinicians are so reluctant to prescribe personalized dosing that the pharmaceutical industry almost never does that.”
The Pharmaceutical Research and Manufacturers of America, the industry’s leading lobbying organization, says the FDA publishes sex differences when appropriate with new drug approvals. “It would not be practical or feasible to power every study to look for differences if the early trials are not showing clear biological differences,” said Jocelyn Ulrich, PhRMA’s deputy vice president for policy and research.
The FDA does have a plan to consider sex at every step of the drug approval process. “We know that disease sometimes manifests differently in women than in men; sometimes women also respond differently to FDA-regulated products,” the plan says.
Failure to recognize this can be deadly.
One of the clearest cases is Ambien, a sleep aid approved in 1992. The FDA was aware from the start that its effects might not wear off by morning, and warned that users might walk and even drive in their sleep. When people taking the drug caused fatal car crashes, the “Ambien defense” became a common courtroom term.
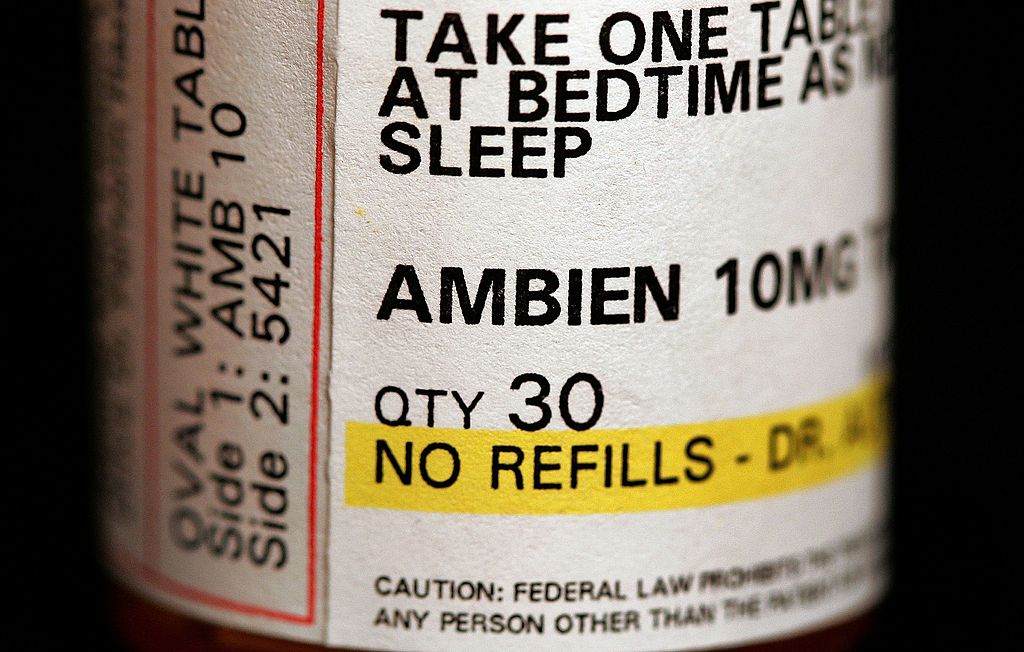
It wasn’t until years later that researchers noticed this problem affected women far more than men because their bodies metabolize the drug differently. In 2018 — more than 25 years after the drug’s approval — the FDA required a lower dose for women.
“We caught Ambien, but there are so many other drugs or therapeutics out there that are not providing outcomes that they did in trials,” said Irene Aninye, chief scientist for the Society for Women’s Health Research.
A 2001 report by the U.S. Government Accountability Office found that eight of the 10 drugs pulled off the market in the previous four years because of potentially deadly side effects were riskier for women than for men.
These included the diet drug fenfluramine, which caused strokes, and the heart drug Posicor, which slowed heart rates in otherwise healthy people, especially elderly women.
A followup by the GAO in 2015 faulted the NIH for failing to do more to make sure it was following its own policies.
Increasing enrollment of underrepresented and excluded populations would require better enforcement of the federal guidance and having more women scientists to conduct research, especially at high levels. “Women, people from diverse backgrounds, ask different questions,” Clayton said.
Some drugs work better in women than in men, including so-called targeted therapies in cancer care, LeBoeuf said. “When you give immunotherapy to melanoma patients, women tend to do better,” she said. “We know very little in terms of the why.”
More research could show whether it’s because of a hormone such as estrogen. And if tweaking hormones during cancer care improves results, that could benefit men as well.
The future of women’s health research
NIH is working on several fronts to improve things, encouraging research institutions to increase diversity among research staff and offering funding to study sex as a biological variable.
The NIH’s All of Us Research Program aims to enroll a greater diversity of people into clinical research with online questionnaires, voluntary DNA sampling by outreach to minority communities. The FDA launched a program this spring to make it easier for various populations to join clinical trials by, for example, expanding them to smaller communities.
The NIH has allocated nearly $1 billion to better coordinate research on autoimmune disease, which disproportionately affects women, Clayton said. It also is working to help women and people of color find funding for scientific research.
“Historically, we’re just getting to a point where women are finally in leadership positions in science. Men have been the leaders and men don’t understand women’s bodies,” said Bethany Young Holt, founder and executive director of CAMI Health, a global women’s health organization focused on sexual and reproductive health.
“They just understand their own.”
Faubion, of The Menopause Society, said that until medical journals require analysis of results by sex, researchers simply won’t do it. “We have a big problem in that journal editors are not making them do this,” she said.
Annette Flanagin, the executive managing editor of JAMA and its network of journals, said they ask researchers to do so, but Faubion said they don’t enforce such requests.
More legislation may be needed, said Schubert, of the Society for Women’s Health Research.
Dr. JoAnn Manson, an epidemiologist at the Harvard T.H. Chan School of Public Health, agrees. She helped lead the biggest-ever study into women’s health, the Women’s Health Initiative. “When the Women’s Health Initiative was started in 1992, it was a line item in the congressional budget,” she pointed out.
First Lady Jill Biden said the new White House initiative is intended to go much further in closing medical treatment gaps between men and women. “Every woman I know has a story about leaving her doctor’s office with more questions than answers. Not because our doctors are withholding information, but because there’s just not enough research yet on how to best manage and treat even common women’s health conditions. In 2023, that is unacceptable,” Biden said.
“We have a clear goal: to fundamentally change how we approach and fund women’s health research.”
***
This article was corrected to say that the NIH has allocated nearly $1 billion to better coordinate research on autoimmune disease, rather than for a new office, as an earlier version said.
